Botox microdroplet injections use botulinum toxin type A to smooth out the skin, improve texture, and reduce shine. Instead of targeting muscles, the toxin is diluted and injected intradermally in tiny aliquots, where it acts on the superficial dermis.
Read on to learn how the Botox microdroplet technique works, the dilution protocols most often used, and how it fits in clinical practice.
Key Takeaways
- The Botox microdroplet technique delivers diluted botulinum toxin into the dermis in tiny aliquots to improve skin quality.
- Unlike traditional Botox, which targets deep muscle groups, microbotox acts on superficial muscle fibers, sweat glands, and sebaceous glands to avoid the “frozen” look.
- The toxin’s mechanism blocks acetylcholine release at the dermal-subdermal junction, which reduces glandular activity and weakens surface muscle fibers.
- Dilution protocols depend on the area being treated. Common solutions are 20 U/mL for oily skin and pores and 28 U/mL (or higher) for jawline and neck tightening.
- Dosing also depends on the area being treated: 20-24 U for pore refinement and up to 74 U for platysmal bands and neck contouring.
- Clinicians inject intradermally in a 1 cm² grid using microdroplets of 0.01 to 0.05 mL.
- Results last three to four months on average, with some patients experiencing up to six months of smoother skin.
What Is the Botox Microdroplet Technique?
Botox microdroplet, also called microbotox, mesobotox, or the Botox facial technique, is an off-label use of botulinum toxin type A.
Instead of large doses directed into the muscle, the toxin is diluted and delivered in multiple, evenly spaced microdroplets placed across the dermal and superficial subdermal layers.1
Microbotox acts on superficial muscle fibers, sweat glands, and sebaceous glands. This way, it can:
- Soften fine lines and rhytides while deeper muscle function remains intact
- Decrease sebaceous and sweat gland activity, which means less oil and sweat production
- Improve skin texture and pore size as glandular activity slows down and the skin envelope tightens
Because of this multi-level effect, the technique is often described as a form of “chemoresurfacing.” It improves skin quality and treats areas that are traditionally difficult with intramuscular injections, like the undereye region, lateral forehead, neck, and jawline.2
Mechanism of Action of the Botox Microdroplet Technique
Microbotox works through the same neurochemical pathway as traditional botulinum toxin type A: it blocks the release of acetylcholine at the neuromuscular junction. Without acetylcholine, muscle fibers cannot contract, and sweat and sebaceous glands cannot secrete normally.
The difference comes from where the neurotoxin is placed and how much of it diffuses into the target structures. When Botox is placed at the dermal-subdermal junction, it diffuses into two main targets:
- Superficial muscle fibers. These fibers are attached to the underside of the dermis and contribute to fine surface rhytides. Microdroplet injections cause mild weakening of these fibers without affecting deeper muscle groups. The result is soft effacement of lines while natural facial movement is preserved.
- Glandular structures. The toxin acts on eccrine sweat glands and sebaceous glands through cholinergic blockade, which leads to reduced sweat and sebum output. Over time, glandular atrophy tightens the skin envelope, decreases pore visibility, and improves surface smoothness.
A third effect sometimes seen is fluid retention in the dermis. Since microdroplet injections relax muscles around lymphatic channels and alter the osmotic balance, they create a temporary “refreshed” look.3
Dilution Protocol for Botox Microdroplets
Different areas of the face and neck respond best to different dilutions. Here’s a general breakdown of how units can be diluted:
| Indication | Suggested dilution | Typical units used |
| Oily skin, enlarged pores, rosacea (T-zone, central face, infraorbital lines) | 20 U in 1 mL saline solution | ~20–24 U total |
| Forehead, glabella, crow’s feet | 24 U in 1 mL solution | ~24 U total |
| Jawline and neck (platysmal bands, horizontal lines, cervicomental contour) | 28 U in 1 mL solution | 56 U for both sides (2 mL), up to 74 U in strong platysmal bands |
| Broad skin refinement | 100 U in 5 mL saline (1 U = 0.05 mL) or 100 U in 10 mL (1 U = 0.1 mL) | 1-5 syringes, depending on the area |
| AbobotulinumtoxinA (ABO, Dysport®) | 300 U in 6 mL saline (≈70 U/mL further diluted) | Variable |
Botox Microdroplet Dosing Guidelines by Facial Zone
Here are the muscles usually injected with microbotox:
1. Forehead
Microbotox in the forehead targets the frontalis muscle, which lifts the brows and causes horizontal forehead lines. It also targets the zones around the glabella and brows to soften lines without a “frozen” look.
A typical protocol uses 24 U spread across 16 points:
- 8 droplets in the glabellar and brow regions to reduce corrugator pull
- 8 droplets around the crow’s feet for smoothness
Each droplet usually contains 0.5 to 1.5 U and is placed intradermally. If patients have already had conventional Botox for brow lifting, the dose is reduced to 12-16 U for maintenance or targeting the lateral forehead.
2. Under-Eye Area
The infraorbital region is one of the most delicate zones for microbotox. Clinicians target the preseptal fibers of the orbicularis oculi to soften fine lines, reduce bunny lines, and improve skin texture under the eyes.
A typical protocol uses 8-12 U of onabotulinum toxin A (ONA), diluted in 0.2-0.3 mL solution. Droplets are placed just below the lash line or along the infraorbital hollow in three to four sites per side. Clinicians can use 1-5 microdroplets of 1-4 U each for lateral canthal lines.
3. Mid-Face
The midface is a sensitive area that requires careful technique because inaccurate placement can cause unwanted effects. Injectors typically use 20 U of onabotulinum toxin A in 1 mL saline for the cheeks and nose.
If the patient requires stronger lifting, some protocols reach up to 50 U per side of ONA, 100-180 U per side of ABO, or 30 U per side of incobotulinum toxin A.
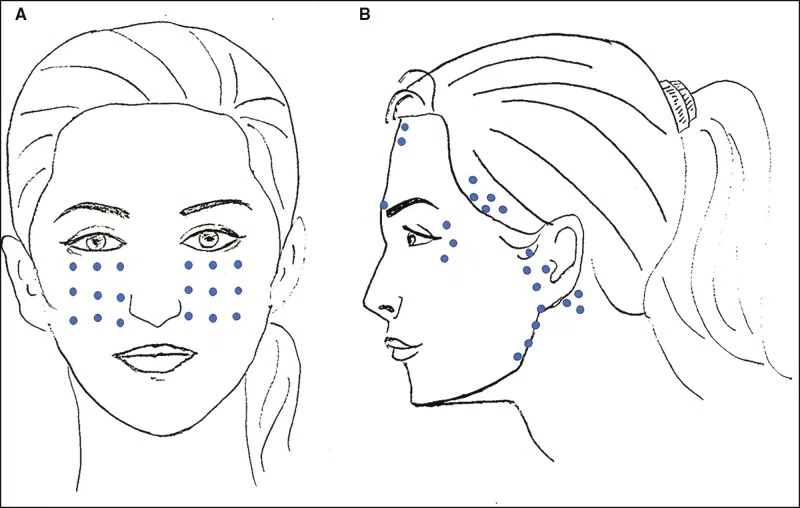
Clinicians usually inject microdroplets in a grid pattern, usually 0.5-1 cm apart across the cheeks. However, they can also place:
- Two rows of droplets over the frontalis
- Two rows at the temples along the hairline
- Several points around the lateral orbicularis oculi, preauricular sites near the tragus, and along the mandibular line at 1 cm intervals
4. Oily Skin
For oily skin, you typically want to inject 20 U of onabotulinum toxin A diluted in 1 mL solution across the T-zone and central third of the face (including the nose) where sebaceous activity is highest.
The effect begins within the first week and lasts up to three to four months.
5. Lower Face and Neck
The lower face and neck are treated to relax the depressor muscles and the superficial fibers of the platysma, which sharpens the jawline and restores a more defined cervicomental angle.
Injectors place microinjections in a grid-like pattern about 1 cm apart, starting two to three finger widths above the lower mandibular border and continuing downward across the anterior neck until the clavicle.
They use a total of 28 U in 1 mL solution and distribute it across one to three syringes, depending on the patient’s neck thickness:
- For patients with thin necks, use 20 U/mL
- For patients with thicker necks, use 28 U/mL or more concentrated dilutions
In some protocols, two syringes (approximately 56 U) are used to cover the entire lower face and neck, with up to three syringes for people with heavier platysmal bands.
Botox Microdroplet Injection Technique
Since every facial zone requires a different concentration and distribution, you need to first decide on the target area before preparing the dilution. That will determine your exact injection technique.
However, here’s how practitioners usually perform microbotox injections:
- Start with a vial of 100 U BoNT-A in 2.5 mL saline.
- In a 1-mL syringe, draw up 0.5 mL, 0.6 mL, or 0.7 mL, depending on the concentration needed. Each syringe provides roughly 100 to 120 microdroplets.
- Dilute with 1 mL saline (or 0.5% lidocaine if preferred) to reach the desired concentration:
- For oily skin, enlarged pores, rosacea, or overall skin refinement, prepare 20 U/mL.
- For dynamic wrinkles in females (forehead, glabella, crow’s feet), prepare 24 U/mL.
- For male wrinkles, neck contouring, or scar prevention, prepare 28 U/mL.
- Apply 5% topical lidocaine to the patient’s skin for 20 minutes, then rinse it off.
- Disinfect the treatment area with alcohol swabs or an antiseptic solution.
- Mark injection points using a 1 cm² grid pattern across the treatment zone:
- On the face, plan for microdroplets from 0.01 to 0.05 mL.
- On the neck, keep droplets smaller (around 0.01 mL) with evenly spaced points.4
- Inject intradermally using a 1-mL syringe with a 30-34G needle.
- Insert the needle into the dermis, going slowly until you see a small bleb with blanching. This confirms proper placement. If the solution flows too easily, the needle is too deep.5
- After injecting each site, withdraw the needle gently to avoid product tracking or bruising.
- Remind patients not to rub, press on, or massage the treated areas for at least four hours.
Source High-Quality Botox With Medica Depot
Microbotox reduces excess oil, minimizes visible pores, and smoothes out skin without the “frozen” look. But these outcomes depend on two factors: your technique and the quality of the product you use.
At Medica Depot, we supply genuine Botox obtained directly from regulated distributors. Our direct manufacturer connections reduce traditional markups and can save you up to 70% compared to local suppliers.
We also back every order with a 100% money-back guarantee, fast international shipping, and dedicated support to help you get exactly what your clinic needs.
If you’re looking to purchase wholesale microbotox at unbeatable pricing, check out our Botox catalog today!
FAQs
1. Who Is an Ideal Patient for Microbotox?
Ideal candidates for microbotox include those with fine lines, oily or acne-prone skin, early signs of aging, as well as people looking for smoother skin and smaller pores without looking “frozen.”
2. Who Is Not a Good Candidate for Microbotox?
Microbotox is not suitable for patients who are pregnant, breastfeeding, have neuromuscular disorders, or have a history of allergy to intradermal botulinum toxin. You should also avoid it if someone has an active skin infection in the treatment area.
3. How Long Does Microbotox Last?
The effects of microbotox typically last three to four months. But some patients may retain results for up to six months, depending on their skin type, treatment area, and lifestyle factors.6
References
1. Wu WTL. The Microbotox Technique. In: Beut FJ, Jelks GW, Lamb J, Lambros V, Surek CC, eds. Centrofacial Rejuvenation: Part II The Place of Toxins and Fillers in the Modern Plastic Surgery Practice. Stuttgart, Germany: Georg Thieme Verlag; 2018. Chapter 11. doi:10.1055/b-0038-149630
2. Kandhari R, Kaur I, Gupta J, Al-Niaimi F. Microdroplet Botulinum Toxin: A Review. J Cutan Aesthet Surg. 2022;15(2):101-107. doi:10.4103/JCAS.JCAS_162_21
3. Malinda IA, Jusuf NK. Skin rejuvenation with Microbotox: a review. J Gen Proced Dermatol Venereol Indones. 2025;9(1):10.
4. Atwa EM, Nasr MM, Ebrahim HM. Evaluation of Intradermal Injection of Botulinum Toxin A for Facial Lifting. J Clin Aesthet Dermatol. 2020;13(12):22-26.
5. Issa MCA, Tamura B (eds). Botulinum Toxins, Fillers and Related Substances. Clinical Approaches and Procedures in Cosmetic Dermatology. Springer Cham; 2016. doi:10.1007/978-3-319-20253-2
6. Wu WTL. Microbotox of the Lower Face and Neck: Evolution of a Personal Technique and Its Clinical Effects. Plast Reconstr Surg. 2015;136(5 Suppl):92S-100S. doi:10.1097/PRS.0000000000001827








